Journal Information
Journal ID (publisher-id): rfoua
Title: Revista Facultad de Odontología Universidad de Antioquia
Abbreviated Title: Rev Fac Odontol Univ Antioq
ISSN (print): 0121-246X
Publisher: Universidad de Antioquia
Periodontal disease (PD) is defined as a multifactorial chronic inflammatory pathology of bacterial origin. The accumulation of plaque around the teeth creates a conducive ecological niche for its growth and development, leading to the destruction of periodontal supporting tissues, compounded by various local and systemic factors. According to a 2010 study conducted by the World Health Organization, approximately 33 % of the global population experiences some form of periodontal disease at some stage in their lives1. Periodontitis, affecting up to 50 % of the worldwide population, can result in severe consequences such as tooth loss2,3. The most prevalent form of periodontal disease is gingivitis, impacting between 30 % and 100 % of the global population(4. Various therapeutic approaches, including oral hygiene, non-surgical periodontal therapy, surgical interventions, and unconventional methods such as the adjunctive use of cannabis, have been proposed for periodontal disease treatment.
Cannabis sativa boasts a medicinal history dating back to 2700 B.C. and is recognized as one of the earliest plants exerting psychotropic effects5. Possessing analgesic, muscle relaxant, antidepressant, hypnotic, immunosuppressive, anti-inflammatory, anxiolytic, and bronchodilator properties, Cannabis sativa extract comprises over 400 chemical components, with at least 60 cannabinoids unique to the species. The three principal cannabinoids-delta-9-tetrahydrocannabinol (THC), cannabidiol (CBD), and cannabinol-exhibit psychoactive effects6. Some studies assert that CBD and other cannabinoids demonstrate potent activity against microorganisms, including methicillin-resistant Staphylococcus aureus, significant contributors to bacterial endocarditis7. Given its anti-inflammatory and antimicrobial attributes, CBD holds promise as a therapeutic adjunct in periodontics. Nevertheless, scant information exists regarding the application of cannabinoids in periodontitis treatment. Consequently, the aim of this systematic review is to ascertain the effects and clinical viability of cannabinoids as an alternative therapeutic option for periodontal disease.
A systematic review was carried out according to the recommendations of the Cochrane manual for systematic reviews. Priority was given to the identification of clinical studies and therefore the following PICO (Patient/Problem, Intervention, Comparator, Outcome) question was formulated:
P: Patients with periodontal disease.
I: Periodontal therapy (prophylaxis or non-surgical therapy) + cannabinoid.
C: Periodontal therapy (prophylaxis or non-surgical therapy), no treatment, placebo, delayed treatment.
O: Changes in periodontal attachment level (CAL) at least 3 months later.
What is the effect of non-surgical + cannabidiol therapy on periodontal attachment levels as compared to conventional non-surgical therapy in patients with periodontal disease?
Additionally, a second, more general question was asked: ¿What are the potential biological and microbiological effects of cannabinoids for the treatment of periodontal disease?
Priority was given in the first phase of evidence identification to randomized controlled clinical trials (RCT) and non-randomized clinical trials (NRCT) evaluating the effect of cannabinoids in the treatment of periodontal disease with a minimum 3-month follow-up. Previous systematic reviews as well as other types of study reviews were not considered. In vitro or animal studies that focused on the microbiological and biological effects of cannabinoids on periodontal cells were accepted for inclusion.
Patients affected by periodontitis (previously chronic or aggressive) with different degrees of severity.
Studies with a follow-up of at least 3 months after the intervention were considered.
Two independent reviewers searched for studies in EMBASE, MEDLINE (PubMed), OVID and The Cochrane Central Register of Controlled Trials (CENTRAL) using keywords and boolean operators. Additionally, the search for gray literature in ScieLo and Google Scholar was complemented. The search period included from the creation of the database until April 2022. A manual search was performed from the reference lists of the included articles. Any discrepancy or difference between investigators was resolved by a third researcher.
(("scaling and root planing"[Title/Abstract] AND "non surgical periodontal therapy"[Title/Abstract] AND "cannabidiol"[Title/Abstract]) OR "CBD"[Title/Abstract]) AND "periodontitis"[Title/Abstract] AND "clinical attachment level"[Title/Abstract] AND "placebo"[Title/Abstract].
There was no language restriction. Articles other than Spanish were translated with a translation service (Google Translate).
Two independent and previously calibrated researchers evaluated the titles and abstracts of potential articles. Articles that passed the initial screening were chosen for full-text review. For both qualitative and quantitative analysis, inclusion criteria were used. Articles that did not meet the inclusion criteria were removed, and the reasons for their removal were given.
Data extraction was performed by two independent researchers using a previously established format. For each study, the following information was collected:
Year of publication, study design, funding source and country of origin.
Participant details including demographic information and inclusion criteria.
Details of the type of intervention.
Details of the control or comparator.
Outcome details: changes in CAL, PD, BoP, adverse effects, biological effect, microbiological effects.
The risk of bias analysis was carried out by two independent evaluators and according to chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions 5.0.1 applying the ROBINS-I tool (Risk Of Bias In Non-randomized Studies - of Interventions) which evaluates the risk of bias in the following domains:
Confusion
Selection of participants
Classification of interventions
Missing data
Results measurement
Selective results report
Overall bias
Each domain is evaluated and determined as risk: low, moderate, serious, critical and no information. For in vitro and animal studies, no analysis of bias was performed.
The data were tabulated and presented as the narrative synthesis of the results since there was not enough clinical studies to perform a meta-analysis.
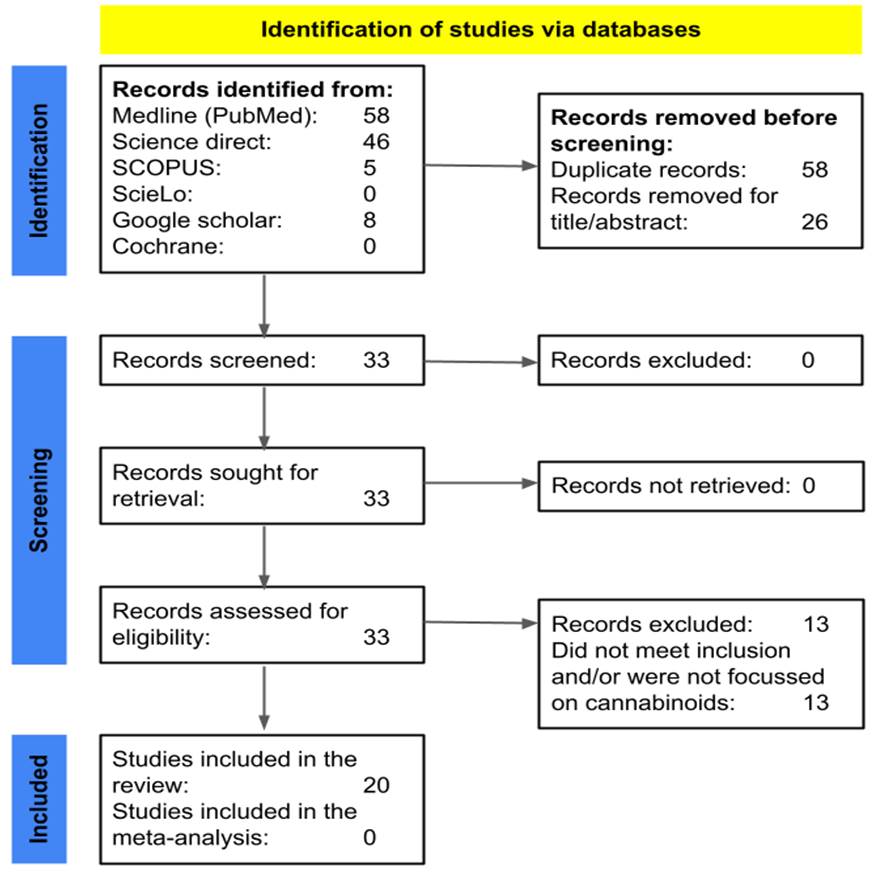
Of a total of 59 potential studies, 26 studies were excluded in the first filter and 33 full-text studies were reviewed. Of these, 13 were excluded for not meeting the selection criteria, leaving a total of 20 studies included in the qualitative synthesis (figure 1). The excluded studies and their reasons are presented in table18-20.
According to the multivariate analysis, the year 2020 presented a negative association only with daily toothbrushing (aPR: 0.97; 95CI%: 0.96-0.99; p<0.001) and toothbrushing minimum twice a day (aPR: 0.96; 95%CI: 0.95-0.98; p<0.001). The year 2021 presented negative association with general toothbrushing (aPR: 0.98; 95%CI: 0.97-0.98; p<0.001), daily toothbrushing (aPR: 0.97; 95%CI: 0.95-0.98; p<0.001) and toothbrushing minimum twice a day (aPR: 0.94; 95%CI: 0.92- 0.96; p<0.001), adjusted for the previously associated covariates (Table 2). These results show that 2021 boasted a lower probability of toothbrushing frequency compared to 2019, considering the three variables used to measure toothbrushing. The same occurred in 2020, except for general toothbrushing, compared to the same reference year.
| Authors | Title | Reason |
| Konermann et al. 20178 | In vivo and in vitro identification of endocannabinoid signaling in periodontal tissues and their potential role in local pathophysiology | Not focused on the use of cannabinoids |
| Ossola et al. 20199 | A new target to ameliorate the damage of periodontal disease: The role of transient receptor potential vanilloid type-1 in contrast to that of specific cannabinoid receptors in rats | Not focused on the use of cannabinoids |
| Gu et al. 201910 | Marijuana-Derived Cannabinoids Trigger a CB2/PI3K Axis of Suppression of the Innate Response to Oral Pathogens | Mixture of animal study and human cells and bacteria. Objective was not clear. |
| Jäger et al. 202011 | Analogous modulation of inflammatory responses by the endocannabinoid system in periodontal ligament cells and microglia | Did not meet inclusion |
| Alvarez et al. 202012 | Long Term Delta-9-tetrahydrocannabinol Administration Inhibits Proinflammatory Responses in Minor Salivary Glands of Chronically Simian Immunodeficiency Virus Infected Rhesus Macaques | Not focused on the periodontal disease |
| Lowe et al. 202113 | The Current and Potential Application of Medicinal Cannabis Products in Dentistry | Review |
| Lowe et al. 202114 | Non-Cannabinoid Metabolites of Cannabis sativa L. with Therapeutic Potential. | Not focused on the use of cannabinoids |
| Lowe et al. 202115 | The Endocannabinoid System: A Potential Target for the Treatment of Various Diseases | Review |
| Blaskovich et al. 202116 | The antimicrobial potential of cannabidiol. | Not focused on periodontal disease |
| Qi et al. 202117 | Evaluation of Cannabinoids on the Odonto/Osteogenesis in Human Dental Pulp Cells In Vitro | Not focused on periodontal disease |
| Aqawi et al. 202118 | Anti-Biofilm Activity of Cannabigerol against Streptococcus mutans | Not focused on periodontal disease |
| Jirasek et al. 202219 | Cannabidiol and periodontal inflammatory disease: A critical assessment. | Review |
| Yan et al. 202220 | The cannabinoid receptor I (CB1) enhanced the osteogenic differentiation of BMSCs by rescue impaired mitochondrial metabolism function under inflammatory condition | Not focused on the use of cannabinoids |
Only one non-randomized clinical study in humans was identified21, which corresponded to a small study in volunteers who underwent prophylaxis with a blaster supplemented with CBD. The results showed a better reduction in microbial counts (linear fold change in the range of 3.9-18.4) with the use of CBD compared to the control (table 2). However, the risk of bias is potentially high due to the study design and conflicts of interest since one of the authors is the founder of the company that manufactured the CBD for the study (figure 2).
| Authors | Objective | Cannabis product | Control | Number of individuals | Results |
|---|---|---|---|---|---|
| Vasudevan & Stahl 2020-Belgium*21 | To determine the possibility of improving supragingival prophylaxis with a blaster supplemented with cannabinoids | Air N Go supplemented with CBD | Air N Go powder | 12 | Reduction in microbial counts (linear fold change in the range of 3.9-18.4) with the use of CBD-supplemented blaster compared to control |
Thirteen in vitro studies reported in table 3 were identified. Treatment of gingival and periodontal fibroblasts with different cannabinoids produced potentially relevant cellular effects for the treatment of periodontitis. A reduction in the expression and production of pro-inflammatory cytokines IL-6, IL-8 and MCP-1 was observed after stimulation with Porphyromonas gingivalis22-26. Quian et al.27 treated periodontal ligament cells with Hu-308 (derived from cannabidiol) and found that it enhances the expression of osteogenic genes and additionally, the differentiation of periodontal ligament stem cells to an osteogenic phenotype28. Other studies reported improvement in the proliferation of gingival fibroblasts and reduction in the production of metalloproteinases29-32. Finally, two studies showed a significant antibacterial effect with CBD treatment33,34. However, they must be considered with care since one of their authors is the founder of the company that manufactured the CBD for the study and therefore represents a conflict of interest. This suggests that cannabinoids have anti-inflammatory and proliferative effects that could have clinical relevance for the treatment of periodontal disease.
| Authors | Cannabis extract / endocannabinoid | Control | Cells / microorganisms | Results |
|---|---|---|---|---|
| Nakajima et al. 2006-Japan22 | AEA | Culture media | HGF | AEA treatment significantly reduced IL-6, IL-8 and MCP-1 production induced by LPS stimulation of P. gingivalis in gingival fibroblasts |
| Qian et al. 2010-China27 | Hu-308 | Culture media | HPLC | Treatment with Hu-308 improved the expression of osteogenic genes in periodontal ligament cells, reflected in an increase in OPG and a reduction in RANKL |
| Kozono et al. 2010-Japan29 | AEA | Culture media | HGF | AEA promotes the proliferation of human gingival fibroblasts |
| Rawal et al. 2012-USA31 | CBD | Culture media | HGF | CBD had little to no significant effect on cell viability. Low CBD concentrations increased TGF-β production by up to 40% while higher concentrations reduced it by up to 40%. CBD increased the amount of fibronectin up to 100% and reduced the amount of MMPs |
| Özdemir et al. 2014-China23 | AEA 2-AG | Culture media | HPLC | AEA showed suppression of gene expression and protein production of IL-8, IL-6 and MCP-1 in fibroblasts stimulated with P. gingivalis. For its part, 2-AG produced an increase in the expression of IL-6, IL-8, and MCP-1. AEA and 2-AG may play important roles in modulating periodontal inflammation, decreasing, or increasing the response, respectively |
| Abidi et al. 2018-USA24 | Endocannabinoides sintéticos SMM-189 y HU-308 AEA | Culture media | HPLF | In the treated fibroblasts there was inhibition in the production of IL-6 and MCP-1. Selective ligands for the CB2R of the endocannabinoid system are effective anti-inflammatory agents for the regulation of periodontal inflammation |
| Lanza Cariccio et al. 2018-Italy30 | CBD MOR | Untreated cells | HPDLSC | Treatment of HPDLSCs with MOR and CBD increased cell survival by inhibiting apoptosis, as demonstrated by increased expression of anti-apoptotic genes and reduction of pro-apoptotic genes |
| Liu et al. 2019-USA32 | THC | Culture media | HPLF | THC promoted adhesion and proliferation of human periodontal ligament fibroblasts |
| Yan et al. 2019-China28 | R‐1 Meth | Culture media | HPDLSC | Treatment with a synthetic endocannabinoid induces the differentiation and proliferation of periodontal ligament stem cells into cells with osteogenic and dentinogenic characteristics through the p38 MAPK and JNK pathway |
| Abidi et al. 2020-USA25 | AEA Hu-308 SMM-189 (agonist) | Culture media | HPLF | AEA produced pro-inflammatory effects. Synthetic drugs dependent on type 2 cannabinoid receptors have an anti-inflammatory effect, demonstrated by a reduction in gene expression and production of proinflammatory cytokines |
| Zhang et al. 2020-Austria26 | Meth-AEA | Culture media | HPLC | Meth-AEA treatment in LPS-stimulated periodontal ligament cells of P. gingivalis significantly reduced the production of IL-6, IL-8, and MCP-1 |
| Stahl & Vasudevan 2020*-Belgium33 | CBD CBC CBN CBG CBGA | Oral B Colgate Cannabite F (pomegranate and seaweed toothpaste) | Plaque culture | Cannabinoids were more effective in reducing bacterial colony counts in plaque bacteria compared to well-established synthetic oral care products such as Oral B and Colgate |
| Vasudevan & Stahl 2020*-Belgium34 | CBD 1% rinse and CBG 1% rinse | CHX 0.2%, alcohol-based rinse and alcohol-free rinse | Plaque culture | In bacterial plaque cultures, CBD rinses had a bactericidal effect similar to that of CHX and reduced total counts |
[i] AEA: Anandamide (Endocannabinoid); HGF: Human Gingival Fibroblasts; THC: Δ‐9‐Tetrahydrocannabinol; HPLF: Human Periodontal Ligament Fibroblasts; CB2R: Cannabinoid Receptor Type 2; CBD: Cannabidiol; CBC: Cannabichromene; CBN: Cannabinol; CBG: Cannabigerol; CBGA: Cannabigerolic Acid; 2-AG: 2-Arachidonylglycerol; HPLC: Human Periodontal Ligament Cells; MOR: Moringin; HPDLSC: Human Periodontal Ligament Stem Cells; MMP: Metalloproteinase; Meth-AEA: Methanandamide; R‐1 Meth: R1 Methanandamide; CB1 and CB2: Cannabinoid Receptor 1 and 2; MAPK: Mitogen-Activated Protein Kinase; JNK: c-Jun N-terminal Kinase; OPG: Osteoprotegerin; RANKL: Receptor Activator of Nuclear Factor Kappa-Β Ligand.
Six animal studies were found and reported in table 4. Treatment with different types of cannabinoids reduced the amount of bone loss in rat models of experimental periodontitis35-38. Similarly, Dronabinol treatment reduced bone resorption on the compression side during orthodontic movement in a rat model39. Lastly, a study in primates reported a reduction in oral microbial dysbiosis and consequently a reduction in gingival inflammation with THC treatment40. This shows an important clinical potential that could be applied to the use in humans.
| Authors | Cannabis extract | Animal model | Results |
|---|---|---|---|
| Napimoga et al. 2009-Brazil35 | CBD | Rats | CBD administration significantly inhibited the volume of bone loss in experimental periodontitis |
| Ossola et al. 2012-Argentina36 | Meth-AEA | Rats | Daily topical treatment with Meth-AEA (500 ng/mL) significantly reduced periodontal bone loss induced by Escherichia coli LPS injection compared to control |
| Ossola et al. 2016-Argentina37 | Hu-308 | Rats | Treatment with Hu-308 had an anti-inflammatory and osteoprotective effect in the development of experimental periodontitis. |
| Ossola et al. 2020-Argentina38 | Hu-308 | Rats | Hu-308 treatment reduced signs of bone destruction in experimental periodontitis |
| McDew-White et al. 2022-USA40 | THC | Primate | THC treatment reduced gingival inflammation and dysbiosis in saliva of treated animals. |
| Klein et al. 2022-USA39 | Dronabinol (synthetic THC) | Rats | THC treatment attenuated orthodontic movement by reducing bone resorption on the compression side of the tooth. |
We conducted a systematic review of the literature to learn more about the effects and clinical applications of cannabinoids as a treatment option for periodontal disease. In total, 20 studies were included (13 in vitro studies, 6 animal studies, and 1 human study), from which important information was extracted and presented in narrative form.
Upon analysis of the results, it becomes evident that each molecule derived from cannabis exhibits a distinct array of effects. For instance, CBD demonstrates bactericidal efficacy, as evidenced by the reduction in bacterial colony numbers in samples of bacterial plaque. Additionally, CBD increases the concentration of fibronectin while concurrently inhibiting apoptosis30,31,33.
THC, for its part, increases gingival fibroblast adhesion and proliferation32, as does AEA, which is also a periodontal inflammation modulator and increases the expression of osteogenic genes by decreasing the production of IL-6, IL-8, and MCP-1(23, 26). This was supported by animal studies in which CBD reduced the volume of bone los35 while also producing an anti-inflammatory effect (reduction of gingival inflammation) and an osteoprotective effect that resulted in decreased bone resorption37. While these biological effects have been documented in preclinical studies, their potential clinical impact holds promise for the treatment of periodontitis. Specifically, cannabinoids may help mitigate periodontal inflammation and consequent clinical attachment loss, impair supragingival and subgingival microbial overgrowth, protect bone tissue, and promote fibroblast proliferation in patients undergoing periodontal treatment and maintenance.
However, after conducting this systematic review for evidence, we found that the use of cannabinoids for periodontitis treatment is not yet clearly scientifically supported. Cannabinoids have demonstrated anti-inflammatory, bactericidal, osteoprotective, and cell-proliferative effects on both cells and bacteria. Still, their application as a therapeutic measure in periodontics remains undetermined, primarily due to the limited quality of the sole human study available and the presence of a conflict of interest. The absence of randomized clinical studies involving cannabinoids in periodontics represents a notable gap in knowledge. Randomized clinical trials are considered the gold standard for assessing the efficacy and safety of medical interventions. Without such studies, the clinical community is left with a limited understanding of the true therapeutic potential and safety profile of cannabinoids in addressing periodontal conditions. Addressing this gap through well-designed randomized clinical trials would contribute significantly to advancing our understanding of cannabinoids' role in periodontics, informing evidence-based practices, and guiding future treatment approaches in a field that continuously seeks effective and innovative therapeutic solutions. Even though there have been few studies, it has been demonstrated in animals and in vitro studies that cannabinoids may have positive periodontal effects.
The available scientific evidence is scarce to recommend the use of cannabis derivatives for the treatment of periodontal disease. Despite promising findings in preclinical studies indicating therapeutic potential, further investigation is required to assess its application in human subjects.
1. ANUIES. Un alto porcentaje de la población mundial padece la enfermedad periodontal [Website]. México: ANUIES - Asociación Nacional de Universidades e Instituciones de Educación Superior; 2005. Available in: https://bit.ly/49zmqzd
3. FDI World Dental Federation. Salud y enfermedades periodontales: guía práctica para reducir la carga mundial de morbilidad para las enfermedades periodontales. FDI World Dental Federation; 2018. Available in: https://www.fdiworlddental.org/sites/default/files/2020-11/gphp-2018-toolkit-es.pdf
8. Konermann A, Jäger A, Held SAE, Brossart P, Schmöle A. In vivo and In vitro Identification of endocannabinoid signaling in periodontal tissues and their potential role in local pathophysiology. cellular and molecular neurobiology. Cell Mol Neurobiol. 2017. 37: 1511-20. DOI: https://doi.org/10.1007/s10571-017-0482-4
9. Ossola CA, Balcarcel NB, Astrauskas JI, Bozzini C, Elverdin JC, Fernández-Solari J. A new target to ameliorate the damage of periodontal disease: the role of transient receptor potential vanilloid type-1 in contrast to that of specific cannabinoid receptors in rats. J Periodontol. 2019; 90(11): 1325-35. DOI: https://doi.org/10.1002/JPER.18-0766
25. Abidi AH, Alghamdi SS, Dabbous MK, Tipton DA, Mustafa SM, Moore BM. Cannabinoid type-2 receptor agonist, inverse agonist, and anandamide regulation of inflammatory responses in IL-1β stimulated primary human periodontal ligament fibroblasts. J Periodontal Res. 2020; 55(5): 762-83. DOI: https://doi.org/10.1111/jre.12765
28. Yan W, Cao Y, Yang H, Han N, Zhu X, Fan Z et al. CB1 enhanced the osteo/dentinogenic differentiation ability of periodontal ligament stem cells via p38 MAPK and JNK in an inflammatory environment. Cell Prolif. 2019; 52(6): e12691. DOI: https://doi.org/10.1111/cpr.12691
30. Lanza Cariccio V, Scionti D, Raffa A, Iori R, Pollastro F, Diomede F et al. Treatment of periodontal ligament stem cells with MOR and CBD Promotes cell survival and neuronal differentiation via the PI3K/Akt/mTOR pathway. Int J Mol Sci . 2018; 19(8): 2341. DOI: https://doi.org/10.3390/ijms19082341
31. Rawal SY, Dabbous MKh, Tipton DA. Effect of cannabidiol on human gingival fibroblast extracellular matrix metabolism: MMP production and activity, and production of fibronectin and transforming growth factor β. J Periodontal Res . 2011; 47(3): 320-9. DOI: https://doi.org/10.1111/j.1600-0765.2011.01435.x
35. Napimoga MH, Benatti BB, Lima FO, Alves PM, Campos AC, Pena-Dos-Santos DR et al. Cannabidiol decreases bone resorption by inhibiting RANK/RANKL expression and pro-inflammatory cytokines during experimental periodontitis in rats. Int Immunopharmacol. 2009; 9(2): 216-22. DOI: https://doi.org/10.1016/j.intimp.2008.11.010
40. McDew-White M, Lee E, Alvarez X, Sestak K, Ling BJ, Byrareddy SN et al. Cannabinoid control of gingival immune activation in chronically SIV-infected rhesus macaques involves modulation of the indoleamine-2,3-dioxygenase-1 pathway and salivary microbiome. EBioMedicine. 2022; 75: 103769. DOI: https://doi.org/10.1016/j.ebiom.2021.103769
[10] García-Gutiérrez L, Hoyos-Castrillón Y, Garcés-Londoño S, Jaimes-Ríos S. Effects and clinical application of cannabinoids for the treatment of periodontal disease: a systematic review. Rev Fac Odontol Univ Antioq. 2023; 36(1): 73-84 DOI: http://dx.doi.org/10.17533/udea.rfo.v36n1a7