Open versus Laparoscopic Splenectomy: Experience at Fundación Cardioinfantil-Instituto de Cardiología, Bogotá-Colombia
DOI:
https://doi.org/10.17533/10.17533/udea.iatreia.v31n3a02Keywords:
hematologic diseases, laparoscopy, splenectomy, splenomegaly, postoperative complicationsAbstract
Objective: To compare laparoscopic and open splenectomy in patients with hemorrhagic splenic pathology.
Methods: A cross-sectional study was conducted, based on an institutional registry of open and laparoscopic splenectomies performed at Fundación Cardioinfantil-Instituto de Cardiología between 1996 and 2016. Preoperative, intraoperative and postoperative variables were assessed; the rate of complications, surgical time, hospital length of stay and the need for reoperation were compared between the approaches.
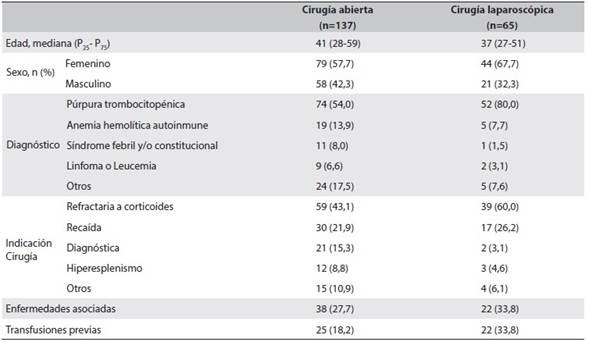
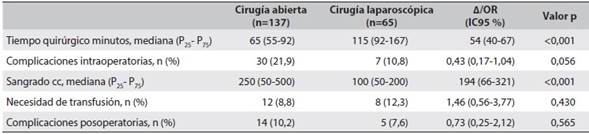
Results: Information of 202 patients was assessed. Open approach was performed in 137 patients (68 %), 61% were men and the median age was 39.5 years (P25-P75 27.7-58.0). Thrombocytopenic purpura refractory to management with corticosteroids was the main indication for surgery. A longer surgical time (median=129 minutes) and less bleeding (median=100 cc P25-P75 50-200) for laparoscopic approach versus open approach (median=60 minutes; median=250 cc P25-P75 50-500, respectively) was identified (p<0.001). Intraoperative complications were similar in both groups (p=0,065), the conversion rate in laparoscopic group was 26.1 %, it was secondary to splenomegaly. No statistically significant differences were found in the two groups in the need for transfusion, hospital length of stay or reoperation.
The rate of postoperative complications was 10.2 % for open splenectomy and 7.6 % for laparoscopic.
Conclusions: Laparoscopic splenectomy is a safe procedure that offers benefits in relation to the open approach for the management of hematological diseases in terms of intraoperative bleeding and is comparable in the identification of supernumerary spleens, surgical complications, and hospitalization time.
Downloads
References
(1.) Mebius RE, Kraal G. Structure and function of the spleen. Nat Rev Immunol. 2005 Aug;5(8):606-16.
(2.) Habermalz B, Sauerland S, Decker G, Delaitre B, Gigot JF, Leandros E, et al. Laparoscopic splenectomy: the clinical practice guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc. 2008 Apr;22(4):821-48. DOI 10.1007/s00464-007-9735-5.
(3.) Katz SC, Pachter HL. Indications for splenectomy. Am Surg. 2006 Jul;72(7):565-80.
(4.) Delaitre B, Maignien B. [Splenectomy by the laparoscopic approach. Report of a case]. Presse Med. 1991 Dec;20(44):2263. French.
(5.) Cordera F, Long KH, Nagorney DM, McMurtry EK, Schleck C, Ilstrup D, et al. Open versus laparoscopic splenectomy for idiopathic thrombocytopenic purpura: clinical and economic analysis. Surgery. 2003 Jul;134(1):45-52.
(6.) Chen J, Ma R, Yang S, Lin S, He S, Cai X. Perioperative outcomes of laparoscopic versus open splenectomyfor nontraumatic diseases: a meta-analysis. Chin Med J (Engl). 2014;127(13):2504-10.
(7.) Winslow ER, Brunt LM. Perioperative outcomes of laparoscopic versus open splenectomy: a meta-analysis with an emphasis on complications. Surgery. 2003 Oct;134(4):647-53; discussion 654-5.
(8.) Campos-Campos SF, Lara-Olmedo JL, Cervantes-Cruz J, Licona-Hernández JC, Delgadillo-Teyer G, Garcés-Monterrubio MG. Esplenectomía en pacientes con enfermedades hematológicas autoinmunes. Estudio comparativo entre técnicas laparoscópica y abierta. Cir Cir. 2007;75(2):75-80.
(9.) Ruiz-Tovar J, Alonso Hernández N, Pérez de Oteyza J, Aguilera Velardo A, Rojo Blanco R, Collado Guirao MV, et al. Esplenectomía laparoscópica o esplenectomía abierta en el tratamiento de la púrpura trombocitopénica idiopática. Cir Esp. 2007 Abr;81(4):192-6. DOI 10.1016/S0009-739X(07)71298-8.
(10.) Pattenden CJ, Mann CD, Metcalfe MS, Dyer M, Lloyd DM. Laparoscopic splenectomy: a personal series of 140 consecutive cases. Ann R Coll Surg Engl. 2010 Jul;92(5):398-402. DOI 10.1308/003588410X12664192076133.
(11.) Zundel N, Arias F, Nassar R. Esplenectomía laparoscópica. Experiencia de 9 años. Rev Mex Cir Endosc. 2002 Abr-Jun;3(2):66-70.
(12.) Maluenda F, Burdiles P, Braghetto I, Csendes A. Esplenectomía laparoscópica en enfermedades hematológicas. Rev Med Chile. 2004 Feb;132(2):189-94. DOI 10.4067/S0034-98872004000200008.
(13.) Patel AG, Parker JE, Wallwork B, Kau KB, Donaldson N, Rhodes MR, et al. Massive splenomegaly is associated with significant morbidity after laparoscopic splenectomy. Ann Surg. 2003 Aug;238(2):235-40.
(14.) Owera A, Hamade AM, Bani Hani OI, Ammori BJ. Laparoscopic versus open splenectomy for massive splenomegaly: a comparative study. J Laparoendosc Adv Surg Tech A. 2006 Jun;16(3):241-6.
(15.) Zhou J, Wu Z, Cai Y, Wang Y, Peng B. The feasibility and safety of laparoscopic splenectomy for massive splenomegaly: a comparative study. J Surg Res. 2011 Nov;171(1):e55-60. DOI 10.1016/j.jss.2011.06.040.
(16.) Koshenkov VP, Németh ZH, Carter MS. Laparoscopic splenectomy: outcome and efficacy for massive and supramassive spleens. Am J Surg. 2012 Apr;203(4):517-22. DOI 10.1016/j.amjsurg.2011.05.014.
(17.) Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004 Aug;240(2):205-13.
(18.) Boddy AP, Mahon D, Rhodes M. Does open surgery continue to have a role in elective splenectomy? Surg Endosc. 2006 Jul;20(7):1094-8.
(19.) Maurus CF, Schäfer M, Müller MK, Clavien PA, Weber M. Laparoscopic versus open splenectomy for nontraumatic diseases. World J Surg. 2008 Nov;32(11):2444-9. DOI 10.1007/s00268-008-9727-1.
(20.) Pietrabissa A, Morelli L, Peri A, Pugliese L, Zonta S, Dionigi P, et al. Laparoscopic treatment of splenomegaly: a case for hand-assisted laparoscopic surgery. Arch Surg. 2011 Jul;146(7):818-23. DOI 10.1001/archsurg.2011.149.
(21.) Feldman LS, Demyttenaere SV, Polyhronopoulos GN, Fried GM. Refining the selection criteria for laparoscopic versus open splenectomy for splenomegaly. J Laparoendosc Adv Surg Tech A. 2008 Feb;18(1):13-9. DOI 10.1089/lap.2007.0050.
(22.) Peters MB Jr, Camacho D, Ojeda H, Reichenbach DJ, Knauer EM, Yahanda AM, et al. Defining the learning curve for laparoscopic splenectomy for immune thrombocytopenia purpura. Am J Surg. 2004 Nov;188(5):522-5.
(23.) Rege RV, Joehl RJ. A learning curve for laparoscopic splenectomy at an academic institution. J Surg Res. 1999 Jan;81(1):27-32.
(24.) Targarona EM, Espert JJ, Balagué C, Piulachs J, Artigas V, Trias M. Splenomegaly should not be considered a contraindication for laparoscopic splenectomy. Ann Surg. 1998 Jul;228(1):35-9.
(25.) Feng S, Qiu Y, Li X, Yang H, Wang C, Yang J, et al. Laparoscopic versus open splenectomy in children: a systematic review and meta-analysis. Pediatr Surg Int. 2016 Mar;32(3):253-9. DOI 10.1007/s00383-015-3845-2.
(26.) Dagash H, Chowdhury M, Pierro A. When can I be proficient in laparoscopic surgery? A systematic review of the evidence. J Pediatr Surg. 2003 May;38(5):720-4.
(27.) Sampath S, Meneghetti AT, MacFarlane JK, Nguyen NH, Benny WB, Panton ON. An 18-year review of open and laparoscopic splenectomy for idiopathic thrombocytopenic purpura. Am J Surg. 2007 May;193(5):580-3; discussion 583-4.
Published
How to Cite
Issue
Section
License
Copyright (c) 2018 Iatreia

This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Papers published in the journal are available for use under the Creative Commons license, specifically Attribution-NonCommercial-ShareAlike 4.0 International.
The papers must be unpublished and sent exclusively to the Journal Iatreia; the author uploading the contribution is required to submit two fully completed formats: article submission and authorship responsibility.